
How to Heal Adductor Tendinopathy For Good
A few years ago, I developed a bad case of adductor tendinopathy which lasted a very long time- over a year and a half! How did it happen? Too many lower body goals and not enough recovery. Heavy back squats, dragon squats, and middle split eccentrics while cutting bodyweight. No surprise there…
There's plenty of information out there on jumpers's knee and achilles tendinopathy, but at the time I really couldn't find much information surrounding groin injuries. So now that I'm pretty much pain-free here is what I've learned.
The most important bit is to not screw up the initial phase of rehab. Prevent it from becoming a chronic issue in the first place. Easier said than done.
Most tendon pain will heal on its own in 3-6 months if you back off and allow it to recover. If it goes on for much longer, then you know you didn't set yourself up for a smooth and natural recovery from the start. Which to be honest, most people who train hard tend to ignore early signs of damage thinking it will just resolve without much intervention. But you live and you learn the hard way of course. Even if you do let it get to the chronic stage there is certainly still hope. You just need to backtrack.
Let's start with some basic anatomy. You have five main adductors
1. Adductor longus (most commonly injured)
2. Adductor brevis
3. Adductor magnus (biggest, with both adductor and hamstring portions)
4. Adductor minimus (often considered the uppermost part of magnus, but some count it separately)
5. Pectineus (functions as a hip flexor and adductor)
6. Gracilis (runs down to the tibia, also assists in knee flexion)
For the most part, the adductors insert at the front of the hip, and will function as hip flexors as well with the exception of the adductor magnus and gracilis, which has a hamstring component. The adductor magnus is one of the largest muscles in the body, after the gluteus maximus and the quadriceps. All the other adductors are quite small comparatively. The adductor magnus is a very good hip extensor and is the primary extensor when peak force is generated in deep hip flexion (squats and deadlifts).
Activation patterns:
The adductor magnus has the best adduction leverage from anatomical position (neutral) moving out into maximum hip abduction. The gracilis tracks the adductor magnus closely with this activation pattern. However, the adductor magnus loses adduction leverage during deeper hip flexion and has greater leverage to adduct in extension. For example: more activation of magnus in a copenhagen plank vs seated hip adduction machine with the hip flexed to 90 degrees.
When the hip is adducted past the midline of the body, the other adductors (longus and brevis) become the muscles with the best relative leverage.
In deep hip flexion the line of pull of adductor longus shifts posterior to the hip joint center so it can act as a weak hip extensor as well
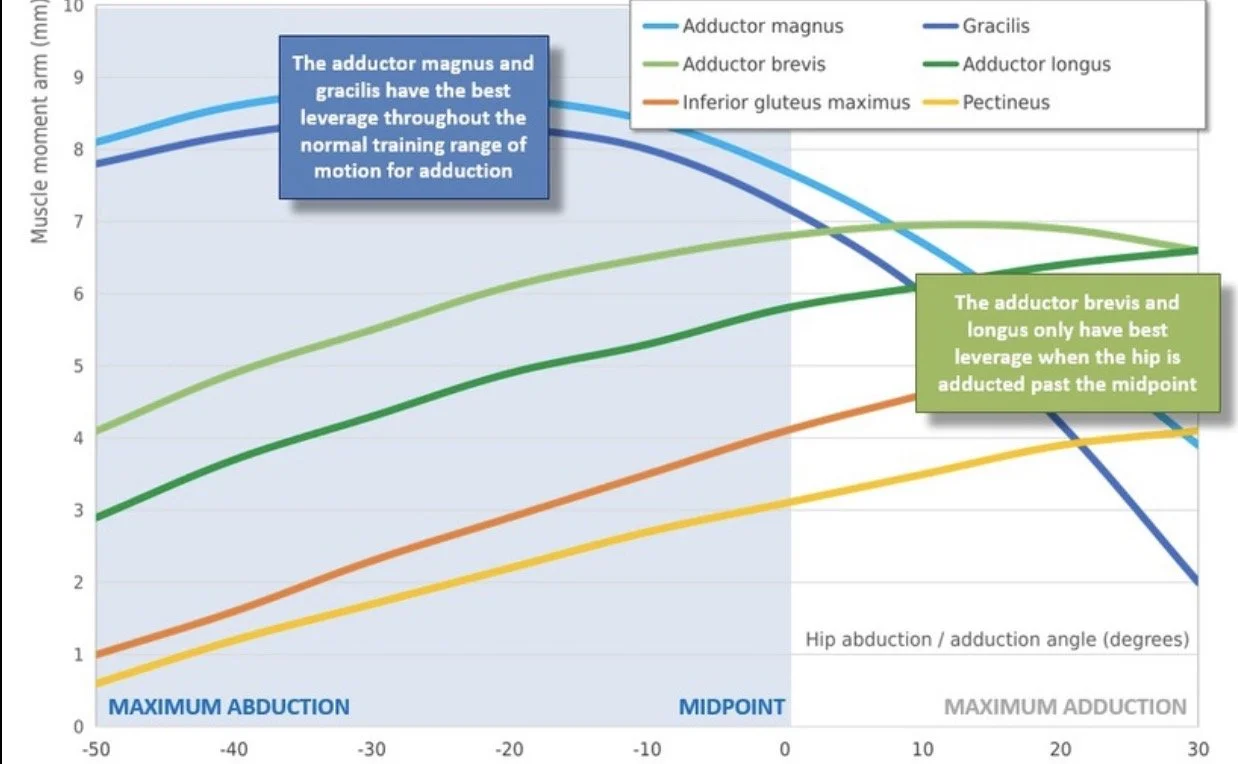
EMG activation patterns- diagram taken from Chris Beardsley
Though the adductors share a common attachment point, The adductor longus tendon is the one most commonly involved in adductor tendinopathy.
It attaches at the pubic bone and is the primary adductor muscle stressed in sports with rapid changes of direction, sprinting, or kicking (e.g., soccer, hockey). Because it handles high loads in hip adduction and stabilization, it’s the most frequent site of chronic groin pain related to tendinopathy. The tendon is also highly innervated with nerves making it painful when injured.
Since the adductor longus is actually a strong hip flexor from an extended position, It's common to feel pain not only when abducting or flexing the hip, but also in deep lunge positions on the back extended leg as well. You may also feel it during core work like hanging leg raises as you are initiating the lift from the bottom. I remember I would feel alot of pain even in a dead bug or plank type exercises
Understanding the functions of the longus is key to guiding our load progressions in the initial stage of rehab.
Here are some general tendinopathy principals:
Load management is key- reducing overall stress of the muscle tendon unit to decrease inflammation and pain
It's important we reduce compressive loads temporarily. Compression refers to mechanical stress placed on a tendon when it’s pressed or wrapped around a bony structure, rather than just being pulled along its length. This often happens when the joint moves into certain angles that “squish” the tendon.
A painful tendon may tolerate loading in one joint angle but flare up in another because of compression. That’s why rehab often starts with loading in non-compressive positions, and only later adds ranges that include compression.
But we should always keep some form of loading at all stages of the rehab process. Tendon injuries respond horribly to rest.
The Adductor longus will be compressed against the pubic bone in deep hip flexion + adduction, as well as in deep hip extension
If you try to research adductor tendinopathy you'll most likely come across the Copenhagen plank. This is where your top foot is placed on a bench in side lying and supporting the weight of your body through the strength of the adductors

I was using this exercise predominantly in the beginning and it's significantly made my pain worse. Even in the most regressed variations.
The problem is the hip is in extension, and the force through adduction is very strong and places a lot of compressive loads on the adductor longus. The copenhagen plank shows very high EMG Activity in the adductors. If the adductors are injured and have low tolerance to force, then a choosing a high force producing exercise is not smart initially.
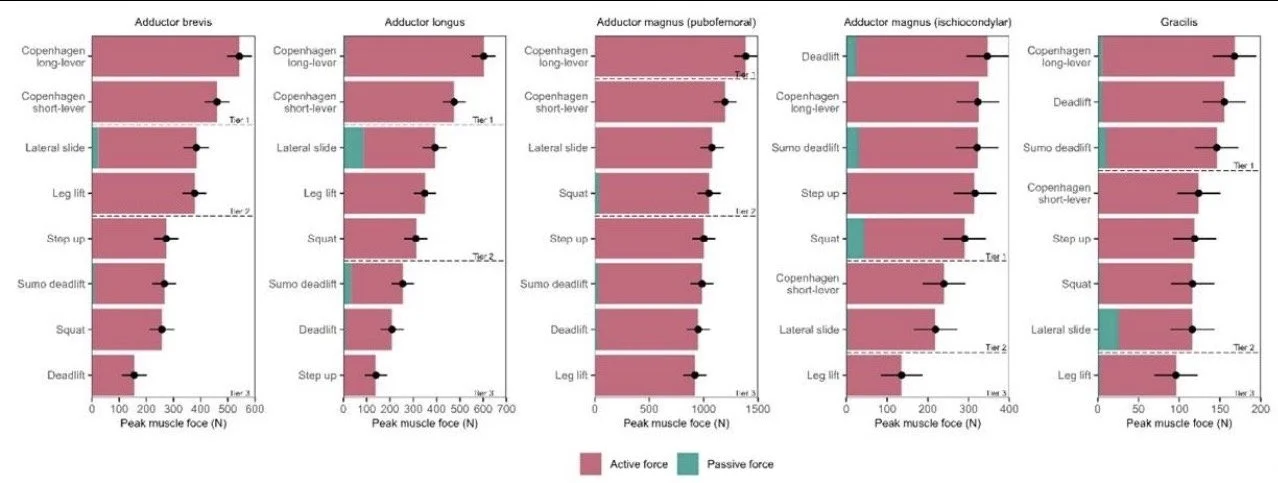
Long lever Copenhagen plank showing the highest EMG activity in all adductors
Often times performing the copenhagen in a bit of abduction with the hip sagged lower to the floor, or in a bit of hip flexion can be more tolerable for an irritated tendon
Initial stages of rehab should avoid end range hip extension AND hip flexion
Also isometrics are overhyped in initial stages of rehab. They can sometimes make things worse. Tendons don't really care about contraction type- just load. The good thing about iso's are they can be self governing and allow you to apply as much internal force as you can currently handle
This is why more overcoming (pushing) type isometrics are more valuable early on than yielding- where you are preventing yourself from lowering (planks, copenhagens,etc)
Here are 3 isometric set ups that work well early on:
Supine/ hooklying ball squeeze

- can be done in varying degrees of hip abduction, flexion, rotation, and extension
Side lying adduction with the hip in 15-20° of hip flexion

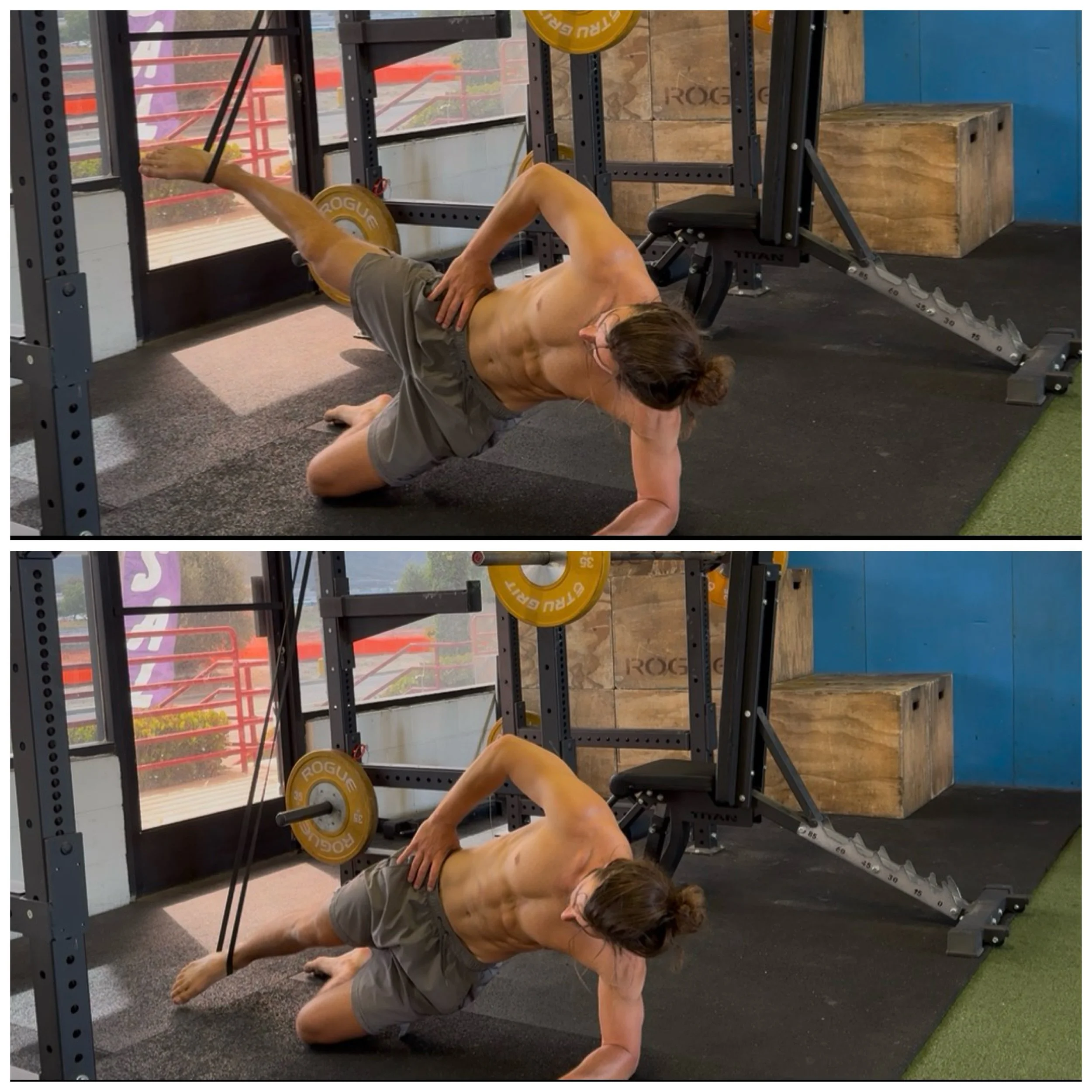
Side Plank Banded Adduction
Seated Straddle Isometric (in varying degrees on abduction depending on what feels best)

If you perform 3 sets of 30-60 seconds and feel better with each subsequent set, this is a good sign your body is responding positively to the loading. If you feel worse after, the force was too high or the angle of laoding is too irritable. Some people respond better with shortened ranges, but for me longer ranges led to greater pain relief (though painful initially).
Sometimes more irritable tendons respond well to shorter duration isometrics for reps around 5-10 seconds, or even on the other end of the spectrum- longer duration with much lighter load around 90-120 seconds to fatigue the muscle without pulling on the tendon. Like I said prior, iso’s aren’t special. Sometimes I wouldn’t do these as a straight static hold but more dynamic through partial ROM for the prescribed time period.
I’m not a fan of daily loading. I prefer to keep these to around 2-3 times a week and allow the other days to just rest it
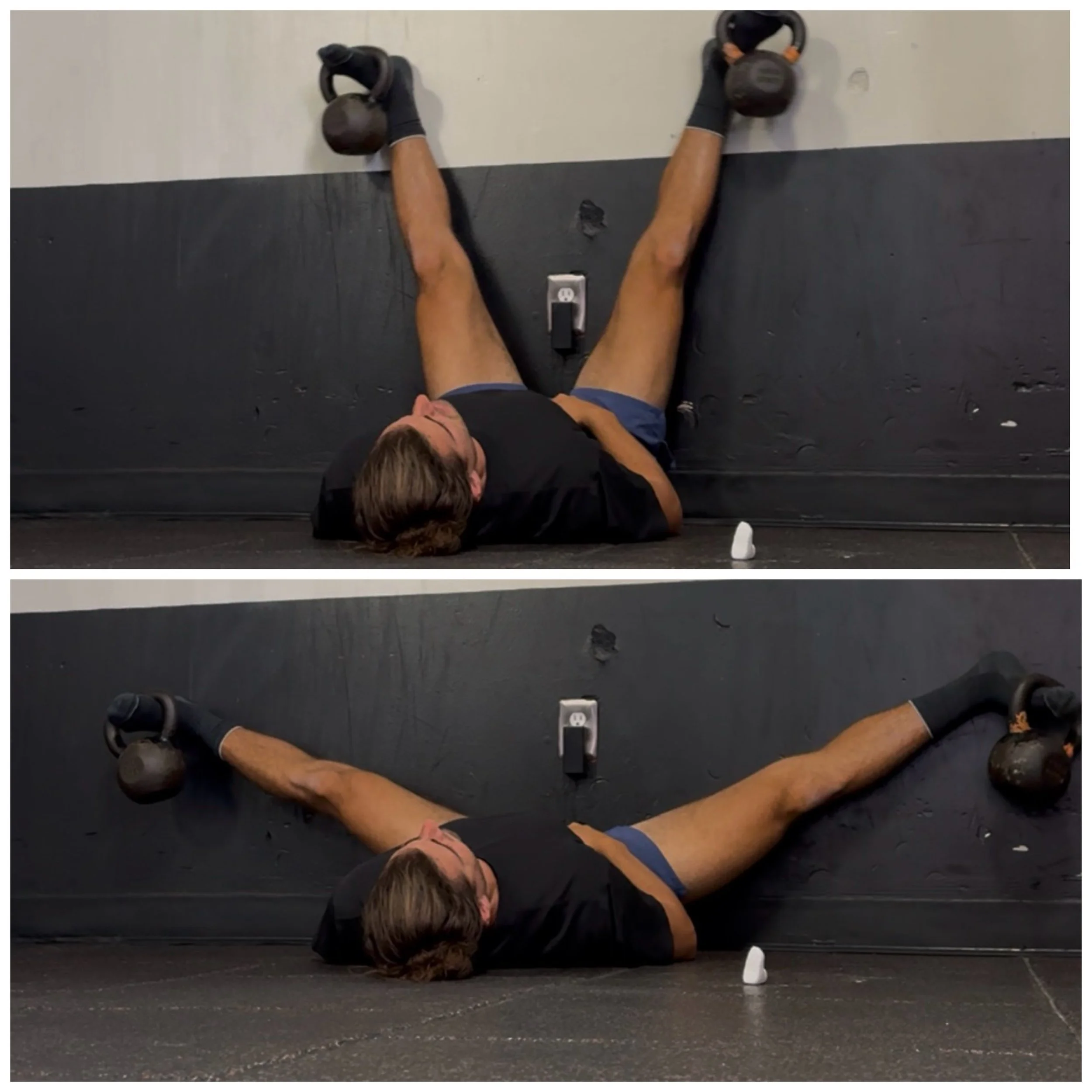
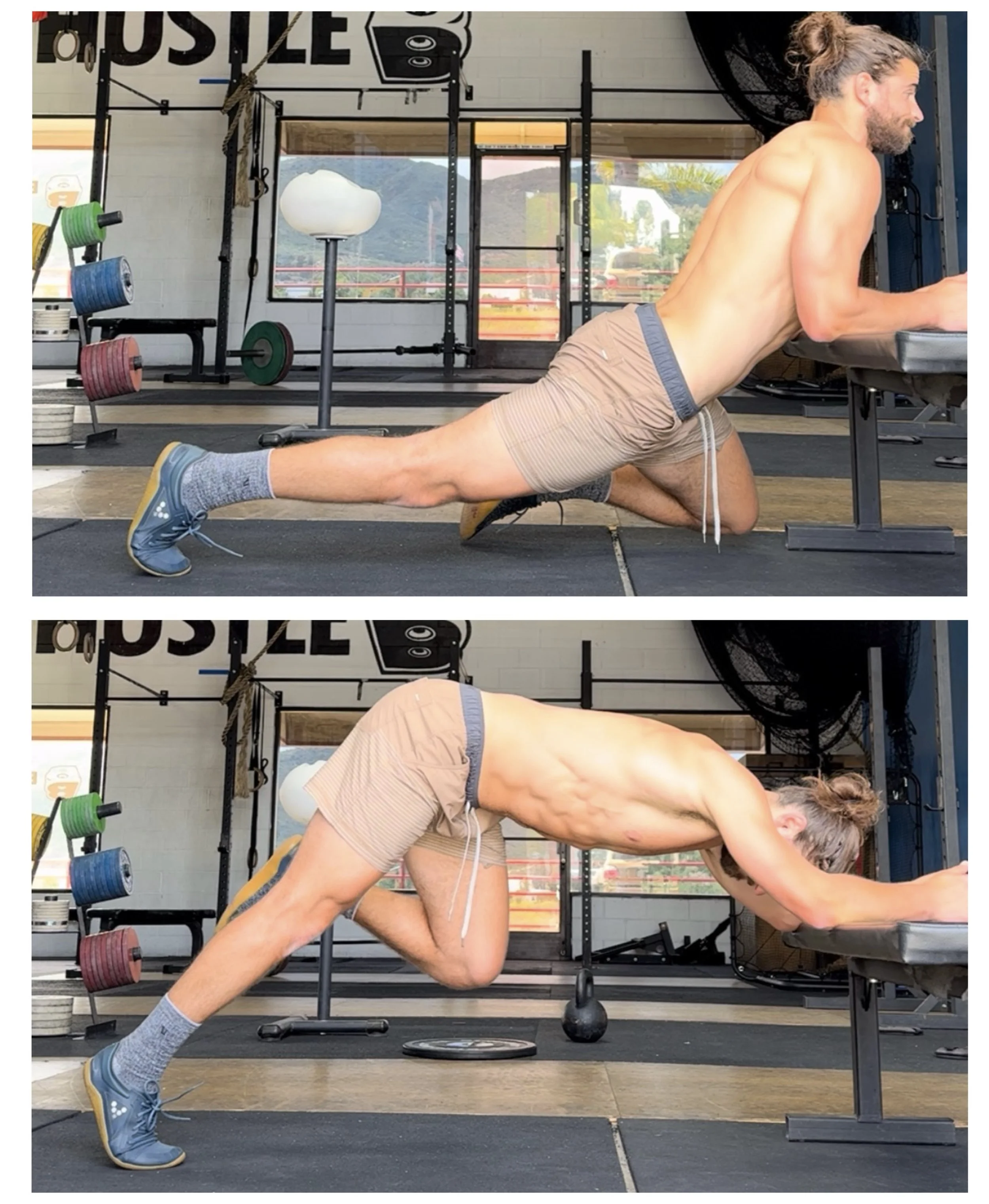
Stage two should include some dynamic loading through range- if you don’t have access to a seated adductor machine, using a wall supported adduction is the next best thing. The wall will keep you at 90° hip flexion which which will start to bias the adductor longus more. You could start with no weight, progress to light ankle weights, then even kettle bells around your toes.
Adductor flies- can be used light weight for high reps, low reps with moderate loads, or low reps with heavy loads just eccentrics
In fact, this was the exercise I predominantly used to rehab my injury. At first, they didn't work as well because I was using them in conjunction with the Copenhagen plank, and deep lunges which were keeping me in a constant state of inflammation
But once I removed the irritable exercises, I was able to benefit from the loading without as much pain. The wall adductor fly biases a more lengthened range for the adductors which surprisingly was more tolerable for me. Lengthened range exercises will typically lead to more structural adaptation in the tendon, but can also be more irritable early on for most other tendon injuries (bicep tendon, patella, hamstring,etc)
It can be beneficial to manipulate tempo with these. Slow eccentrics, pauses just above painful ranges, and even slow concentrics. With this exercise, if the stretched position is the most painful, it should decrease as you warm up into it. Perform this twice a week on days you train lower body
I also enjoyed a few exercises I came up with based on what felt good.
Single leg hip flexor plank raises to target the hip flexor component of the adductor longus, and abdominal fascial connection
And floor Copenhagen isometrics in the lengthened range. At this stage, short range was still quite painful for me, but when I held the position in the stretched position, it made the pain better along the duration of the hold and with each subsequent set

During this stage a bit of pain is fine but we need to monitor our response to loading 24 to 72 hours afterwards. Tendon pain tends to sneak up on you so even though a day after feels fine sometimes it feels even more sore two or three days after. These are still signs that you did too much the session prior.
Lets talk about exercise modification. We want to continue strength training, but make sure we're doing so in a way that keeps the groin muscles loaded but not further irritating the tendon.
It’s common to want to choose unilateral exercises in times of injury because you use lower load overall, but thats actually detrimental with adductor tendinopathy. Unilateral exercises have more of a frontal plane component due to shifting that happens at the hip as well as the increased instability. This makes the adductors work way harder in unilateral compared to bilateral exercises.
Of course heavy deep squats will still be compressive and irritable on the longus tendon but I think squatting to a reduced depth is still a fantastic option to keep in and still train heavy. Back or front Box squatting to 75-90° depth is typically tolerated well
Hinging exercises like RDLs, goodmornings, 45° back extensions, and even hip thrusts are all still fair game
You can even do some lighter full range of motion squatting with a more upright torso as a way of biasing the quads more as long as it's not as hip dominant- hack squats, heel elevated goblet squats, or spanish squats are good options

High Bar, Narrow Stance Squats
Stage 3- bring back compression
Eventually, we need to bring back exercises that caused the most pain in the first place. So we can call this the "bulletproofing" phase. Most people use exercises that are preventative in nature because they strengthen vulnerable angles of the muscle way too early on. This is what screws up the rehab, and turns it into a chronic disaster. We see this in knee pain cases where people use ATG split squats and sissy squats to heal her knees, but it just makes their overloaded knees worse. Those are great exercises to use eventually, they probably needed less compressive exercises on the patellar tendon at first.
Once we have very little pain in stage two exercises, this is where we start loading copenhagen planks, heavier eccentric loading through half split slide outs and wall KB split, and add back in unilateral exercises like high step ups, bulgarian split squats, cossack squats, and deep pause squats. Just not all of this at once. You don't want to make the same mistake that got you a tendinopathy in the first place.


Go with lower reps and still opt for slow eccentrics
3-5 sets of 4-8 repititions 1-2 times a week is great
How long each phase will last is dependent on the person and each unique condition. I also wouldn’t look at the stages as black and white. With tendons, each stage of healing is kind of happening all at once… as confusing as that sounds. For example, you can still have inflammation occuring in a chronic injury- also known as a flare up. In this case, you’ll need to revert back to stage one exercises and reduce compression even if you are 9 months into the injury. Just make sure you don’t progress load too quickly.
Adductor tendon injuries are problematic due to how long they can potentially last, so it is important to stay optimistic. Program modification is necessary to allow you to continue training with intensity, without worrying about the injury. If you have to warm up excessively and psych yourself up to train through the pain, then that is a sign the exercises in your program need to be swapped out. Allow other muscles to take the forefront while the adductors heal, while still loading them enough to keep inflammation and swelling at bay.
Calm shit down, build shit back up. Enough said.